By Dr Pranab Gyawali, Consultant Gastroenterologist (UK-trained) in Dubai
One of the biggest mistakes in Crohn’s disease and ulcerative colitis is assuming that all inflammation is the same.
It is not.
This is one of the key ideas I describe in the video below. Two patients can have the same diagnosis, but the immune pathway driving their inflammation may be different. That is one reason why one biologic may work very well for one person but not for another.
The future of IBD treatment is not just having more medicines. It is choosing the right pathway earlier.
Watch the video
In this short video, I explain why Crohn’s disease and ulcerative colitis treatment is moving toward pathway based thinking.
What does it mean when we talk about IBD pathways?
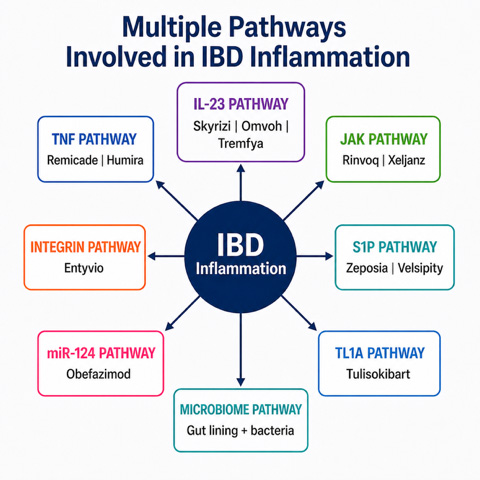
In Crohn’s disease and ulcerative colitis, inflammation can be driven by different immune signals and gut related mechanisms.
Some patients may be more TNF pathway driven.
Some may be more IL-23 pathway driven.
Some may involve JAK signalling, integrin pathways, S1P signalling, TL1A, miR-124, or a combination of several pathways.
The microbiome and the gut barrier may also influence how inflammation behaves.
This matters because biologics and newer IBD medicines do not all work in the same way. They target different parts of the inflammatory process.
Why can one biologic work for one patient but not another?
A biologic works by targeting a specific part of the inflammatory process.
If that pathway is important in one patient, the medicine may work very well. If another pathway is more important, the same medicine may have a weaker effect.
For example, if a patient’s inflammation is strongly TNF driven, an anti-TNF medicine such as infliximab or adalimumab may work well.
If another patient’s inflammation is more IL-23 driven, a medicine such as Skyrizi, Omvoh or Tremfya may be more relevant.
If the disease is mixed, one treatment pathway may not explain everything.
This is why IBD treatment can still feel like trial and error. We have many effective medicines, but we are still not perfect at predicting which treatment is most likely to work before starting.
Why do some patients not respond to biologics?
Biologics can be very effective in Crohn’s disease and ulcerative colitis, but they do not work for everyone.
There are several possible reasons:
- The drug may not be targeting the dominant pathway driving inflammation.
- The disease may involve several pathways at the same time.
- The drug level may not be enough.
- Antibodies may develop with some biologics.
- The disease may have progressed structurally, especially in Crohn’s disease.
- Symptoms may be coming from another issue, such as infection, IBS overlap, bile acid diarrhoea, SIBO or scarring.
This is why I do not like simply saying that a biologic has “failed” without first reassessing what is really happening.
The better question is:
Did we target the right pathway, at the right time, in the right patient?
What does recent research show?
Recent research supports the idea that targeting specific pathways can produce long-term benefit in Crohn’s disease and ulcerative colitis.
In Crohn’s disease, the GALAXI 1 trial reported five-year data with guselkumab, also known as Tremfya. The study showed sustained clinical and endoscopic benefit in many patients through week 240. But not every patient responded fully, which reminds us that other factors and other pathways may still be involved.
In ulcerative colitis, the QUASAR long-term extension showed sustained benefit with Tremfya through week 140, including long-term clinical, endoscopic and histologic outcomes. Again, this is important positive data, but it does not mean every patient will respond in the same way.
The point is not simply that Tremfya works.
The bigger point is that the IL-23 pathway is clearly important in Crohn’s disease and ulcerative colitis.
But the next question is more important for patients:
Who is most likely to respond before we start the treatment?
Can we predict which biologic will work?
Not perfectly yet.
At the moment, treatment choice still depends on several factors, including:
- Disease severity
- Disease location
- Previous medicines
- Previous loss of response
- Safety profile
- Other conditions such as arthritis, psoriasis or liver disease
- Patient preference
- Clinical judgement
But research is moving toward better prediction.
One recent ulcerative colitis study looked at Omvoh, also known as mirikizumab. It found that baseline blood and tissue eosinophil patterns were associated with better clinical and endoscopic outcomes.
This does not mean eosinophils are now a perfect test.
They are not.
But it shows the direction of travel. Researchers are looking for clues before treatment starts, rather than waiting months to see whether the drug has worked.
Can one blood test choose the best biologic?
This is one of the questions patients increasingly ask.
The honest answer is no, not yet.
At present, we do not have one routine blood test that can say with confidence which biologic will work best for most Crohn’s disease or ulcerative colitis patients.
Some markers can help us monitor disease activity. These include blood tests such as CRP, stool tests such as faecal calprotectin, drug levels for some medicines, endoscopy, imaging, and sometimes tissue assessment.
But predicting response before treatment starts is harder.
This is why newer research is looking at combinations of signals, including blood markers, stool markers, tissue markers, microbiome patterns and molecular signatures.
Why does this matter for patients?
Because trial and error costs time.
If a patient spends months on a treatment that is not targeting the right pathway, inflammation may continue silently.
That can mean ongoing symptoms, steroid exposure, repeated flares, hospital admissions, nutritional problems, anaemia, fatigue, and sometimes progression of disease.
The goal is not simply to use stronger drugs.
The goal is to use the right drug, for the right patient, earlier.
What should patients take away from this?
The same diagnosis does not mean the same inflammatory pathway.
This is why one biologic may work brilliantly for one Crohn’s or ulcerative colitis patient but not for another.
The future of IBD treatment is moving toward a more precise model:
Find the dominant pathway, if there is one.
Choose treatment more intelligently.
Reduce months of trial and error.
At present, this is still not possible with routine available tests in the majority of patients. We cannot yet do one simple blood test and say with confidence which biologic will work best.
But this is where research is heading: using blood, stool, tissue, microbiome and molecular signals to better understand which pathway is driving inflammation in each patient.
That is where I believe Crohn’s disease and ulcerative colitis treatment is heading.
Frequently Asked Questions
Why do biologics work for some IBD patients but not others?
Biologics work by targeting specific inflammatory pathways. If that pathway is important in one patient, the drug may work very well. If another pathway is driving the disease, the response may be weaker.
What are the main IBD treatment pathways?
Important pathways include TNF, IL-23, JAK signalling, integrin, S1P, TL1A, miR-124, and the gut barrier or microbiome pathway.
Can a blood test tell me which biologic will work?
Not reliably yet. Some blood, stool, tissue, microbiome and molecular markers are being studied, but there is no single routine blood test that can perfectly choose the best biologic for most Crohn’s disease or ulcerative colitis patients.
What are IL-23 drugs?
IL-23 drugs target one of the important inflammatory pathways in IBD. Examples include Skyrizi, Omvoh and Tremfya.
What are anti-TNF drugs?
Anti-TNF drugs target the TNF inflammatory pathway. Examples include infliximab, adalimumab and golimumab.
What is the JAK pathway?
The JAK pathway is an internal immune signalling pathway. Medicines such as Rinvoq and Xeljanz affect this pathway.
Does a biologic not working mean the disease is worse?
Not always. It may mean the treatment is not targeting the dominant pathway, the drug level is not enough, or symptoms are coming from another issue. This needs proper reassessment rather than guessing.
Can a biologic work at first and then stop working?
Yes. A biologic may lose effect because drug exposure becomes too low, antibodies develop with some medicines, inflammation becomes more active, or another inflammatory pathway becomes more important.
Should I change biologic if I am in remission?
Not without a clear reason. If you are in deep remission, changing treatment may risk losing control. Treatment changes should be based on symptoms, inflammation markers, endoscopy, imaging, safety and specialist judgement.
Recommended Guides for Biologics, Crohn’s and Colitis
1. Understanding IBD
- Why has my biologic stopped working?
- AI in Crohn’s and Ulcerative Colitis: Can Machine Learning Predict IBD Treatment Response?
- JNJ-4804 and dual biological pathway blocking in IBD
- Crohn’s Disease – Symptoms, Tests & Treatment in Dubai
- Ulcerative Colitis – Symptoms, Tests & Treatment in Dubai
- How Biologics Work in Crohn’s & Colitis
- Crohn’s & Colitis: Why You Shouldn’t Stay on Steroids
- Is Your Gut Really Healed? Understanding Deep Remission
- Ulcerative Colitis Progression in Dubai
- Rectal Bleeding
- SIBO in Crohn’s & Ulcerative Colitis
2. Choosing the Right Advanced Treatment
- The new miR-124 treatment pathway
- Next generation stool test in IBD: Granzyme A explained
- New TL1A inhibitor (tulisokibart) – can response be predicted before treatment?
- CAR-T Therapy in Crohn’s Disease – What Patients Need to Know
- Predicting Biologic Treatment Success in Crohn’s & Ulcerative Colitis
- Stelara vs Skyrizi Crohn’s Study Explained
- Tremfya (Guselkumab) Explained
- Tremfya (Guselkumab) in Ulcerative Colitis: Does It Keep Patients Well Long Term?
- Rinvoq – How It Works for Crohn’s & UC
- Predicting Vedolizumab Response Early in IBD
- Vedolizumab in Crohn’s Disease: Why Timing May Change Results
- Icotrokinra: Oral IL-23 Therapy for Crohn’s and Ulcerative Colitis?
- Crohn’s Surgery vs Infliximab in Dubai
- Biologicals & Pregnancy
- 5-ASA – Why It Still Matters
3. Diet, Microbiome and Treatment Response
- Should you avoid dairy in Crohn’s and ulcerative colitis?
- Diet, inflammation monitoring and IBD flare risk
- How the Oxygen Trap May Be Driving Your IBD — And Why Diet Still Matters
- Diet, Microbiome & IBD
- What Leaky Gut Really Means in IBD
- Top Leaky Gut Supplements
- Stress & the Gut–Brain Axis in IBD
- Aloe Vera for Crohn’s & UC
- Black Cumin Seed Oil for IBD
- Vitamin D & Gut Health
- Supplements & Gut Health
- Gluten & IBD — Any Connection?
- Curcumin & Qing Dai in Ulcerative Colitis
4. Tests, Monitoring and Safety
- Flu Vaccines for IBD Patients on Biologics
- Iron Deficiency & Anaemia in IBD
- B12 & Folate Deficiency in IBD
- Colonoscopy
- Capsule Endoscopy
- Diagnostic Tests for Gastrointestinal Disorders
- Hydrogen & Methane Breath Test
- Gut Microbiome Test
- MRI Abdomen / MR Enterography
- CT Abdomen / CT Enterography
If you wish to discuss this further or would like to make an appointment, please use the booking form on this page. Expect a response within 12 business hours.