By Dr Pranab Gyawali, Consultant Gastroenterologist (UK-trained) in Dubai
Early DDW 2026 research on a new investigational medicine designed to block both TNF-alpha and IL-23 pathways in Crohn’s disease and ulcerative colitis.
In my previous VLOG, I discussed one of the most important ideas in modern Crohn’s disease and ulcerative colitis care: the same diagnosis does not always mean the same inflammation.
You can watch that fuller explanation here: Why Biologics Work for Some IBD Patients and Not Others.
That previous VLOG explains why one biologic may work very well for one patient, while another patient with the same diagnosis may need a completely different approach.
This follow-up VLOG looks at an early DDW 2026 study on a new investigational medicine called JNJ-4804, also known as JNJ-78934804.
For those who want to read more about the study itself, the J&J summary is here: JNJ-4804 DDW 2026 study summary.
The reason it caught my attention is simple. It targets two major IBD inflammation pathways at the same time: TNF-alpha and IL-23.
That immediately brings us back to the key question: are we treating the right pathway in the right patient?
What are the different pathways involved in IBD inflammation?
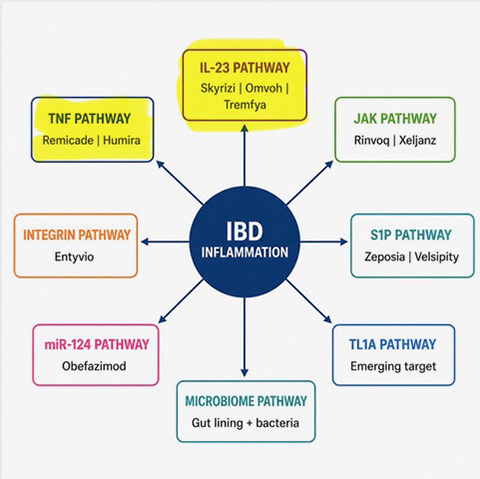
Different inflammatory pathways may be involved in Crohn’s disease and ulcerative colitis.
Crohn’s disease and ulcerative colitis are diagnostic labels.
But underneath those labels, the immune system may be behaving differently in different patients.
Some patients may have inflammation where the TNF pathway is very important. That is why anti-TNF medicines such as infliximab and adalimumab can work very well in some people.
Other patients may have inflammation where the IL-23 pathway is more relevant. Others may involve JAK signalling, gut-selective immune traffic, S1P, TL1A, the gut lining, the microbiome, or a mixture of several pathways.
This is why biologic choice should not be random. The diagnosis matters, but the pathway may matter just as much.
What was different about this new DDW 2026 study?
The early DDW 2026 study looked at JNJ-4804, an investigational treatment designed to block two pathways together: TNF-alpha and IL-23.
This is not the same as simply prescribing two separate biologics side by side.
JNJ-4804 is being developed as one fixed co-antibody treatment, given as a single subcutaneous injection, designed to target both IL-23 and TNF-alpha pathways together.
That distinction matters. This is not routine dual biologic therapy. It is a purpose-built investigational treatment being tested in clinical trials.
Who were the patients in the study?
The patients had moderately to severely active Crohn’s disease or ulcerative colitis.
Many had already had difficulty with previous systemic therapies, including biologics and targeted oral treatments.
Approximately half of participants had already had an inadequate response to two or more therapy classes. That means this was a highly treatment-experienced group, not a simple early treatment group.
This is why the study is clinically interesting. It looked at patients whose Crohn’s or colitis had already been harder to control.
Did it work?
In this early Phase 2b data, yes, there was an encouraging signal.
In Crohn’s disease, about 51% of patients receiving JNJ-4804 reached clinical remission at week 48. The reported endoscopic response rate was about 38%.
In ulcerative colitis, about 41% of patients receiving JNJ-4804 reached clinical remission at week 48.
The treatment was compared with the individual pathway blockers, guselkumab and golimumab, and showed higher clinical and endoscopic outcomes in the J&J summary.
For patients, the simple message is that in harder-to-control IBD, blocking one pathway may sometimes be too simplistic.
But that does not mean every patient needs two pathways targeted. It means we need better ways to understand the biology of each patient.
Is this treatment available now?
No.
JNJ-4804 is still investigational.
The results were presented at DDW 2026 in Chicago as conference data. They are not yet a full peer-reviewed publication, and larger Phase 3 studies are now being initiated.
That matters because early data can look promising, but Phase 3 trials are where we learn much more about effectiveness, safety and which patients benefit most.
What about safety?
The early report stated that safety findings were generally consistent with the known profiles of the individual component treatments.
But this needs caution.
If we block two immune pathways together, long-term safety becomes a major question.
The key issues will be infection risk, longer-term immune effects and whether the benefit is strong enough to justify the extra pathway blockade.
So this is interesting, but it is not something to overstate yet.
Is this the same as dual biologic therapy?
No, not exactly.
Dual biologic therapy usually means prescribing two separate biologic medicines at the same time.
This study was different. It tested one investigational co-antibody treatment designed to target both pathways together in one injection.
It was not directly compared with using two separate biologics side by side.
That question will probably become important in future research, but it was not the central question here.
Why does dual pathway blocking matter?
The main message is not just about one new medicine.
The main message is that pathways are becoming more important in Crohn’s disease and ulcerative colitis.
If inflammation is mainly driven by TNF-alpha, then targeting TNF may make sense. If IL-23 is more important, then an IL-23 approach may be more logical.
But in some patients, especially those whose disease has been harder to control, more than one pathway may be relevant at the same time.
This is where dual pathway blocking becomes scientifically interesting.
It raises the possibility that some patients may not fail treatment simply because the drug was weak. They may fail because the wrong pathway was targeted, the disease biology changed, or several inflammatory signals were active together.
What remains difficult in real clinical practice?
The difficult question is still this: how do we know which pathway is active in which patient?
That is the part we have not fully cracked.
At the moment, we often choose biologics based on disease severity, previous response, safety profile, patient preference, extra-intestinal symptoms and clinical experience.
But the field is moving towards something more precise.
Can we predict the active pathway before choosing the drug?
That is why I think pathway-based thinking is going to become more central in IBD care.
Could there be an earlier immune switch?
There is also a deeper question.
Are TNF-alpha, IL-23, JAK, TL1A and other pathways separate problems, or are they downstream signals from something even earlier in the immune system?
If there is an earlier immune switch that drives several downstream inflammatory pathways, that may be one of the most important areas for future IBD research.
For now, we do not have that answer. But this is why the pathway discussion matters.
What should patients take away?
Patients should not rush to ask for JNJ-4804.
It is not approved yet.
But patients should understand the bigger lesson.
If one biologic does not work, it does not always mean biologics do not work.
It may mean the wrong inflammatory pathway was being targeted.
It may mean the disease biology has changed.
Or it may mean more than one pathway is active.
That is why modern IBD care is increasingly about matching treatment to the biology of the disease, not just the name of the diagnosis.
The future question is not only which biologic should we use. It is also which inflammatory pathway are we trying to treat?
That is why this DDW study is interesting. Not because it gives us all the answers, but because it reinforces the direction IBD care is moving in.
Frequently asked questions
What is dual biological pathway blocking?
Dual biological pathway blocking means targeting two inflammatory pathways involved in IBD at the same time. In this case, JNJ-4804 is designed to target TNF-alpha and IL-23.
Is JNJ-4804 approved for Crohn’s disease or ulcerative colitis?
No. JNJ-4804 is still investigational. The data discussed here came from DDW 2026 conference presentations, and larger Phase 3 studies are still needed.
Is this the same as taking two biologics together?
No. This study tested one investigational co-antibody treatment designed to target two pathways in one injection. It did not directly compare JNJ-4804 with prescribing two separate biologics side by side.
Why are TNF-alpha and IL-23 important?
TNF-alpha and IL-23 are two important inflammatory pathways in IBD. Some current biologics already target these pathways separately. JNJ-4804 is being studied because it targets both together.
Should patients ask their doctor for JNJ-4804 now?
No. It is not approved for routine clinical use. The useful message for patients is to understand that IBD treatment is becoming more focused on pathways and treatment prediction.
Recommended Guides
- The new miR-124 treatment pathway
- Why Biologics Work for Some IBD Patients and Not Others
- Learn about Biologicals used in UC and Crohn’s in Dubai
- Crohn’s Disease Symptoms, Tests and Treatment in Dubai
- Ulcerative Colitis Symptoms, Tests and Treatment in Dubai
Related IBD Treatment and Biologics VLOGs
- How biologics work in Crohn’s and colitis
- Predicting biologic treatment success in Crohn’s and ulcerative colitis
- Stelara vs Skyrizi in Crohn’s disease
- Tremfya in Crohn’s and ulcerative colitis
- Rinvoq and biologics in IBD
- Vedolizumab response prediction
- Biologics and pregnancy in IBD
- Why not to stay on steroids in Crohn’s and colitis
Lifestyle, Microbiome and Pathway-Related Topics
- Diet and microbiome influence on biologic response
- Gut microbiome in Crohn’s and ulcerative colitis
- SIBO in Crohn’s and ulcerative colitis
- Leaky gut in IBD
- Vitamin D and gut health
- Supplements and gut health
Investigations and Procedures
- Colonoscopy in Dubai
- Capsule endoscopy in Dubai
- Diagnostic tests for gastrointestinal disorders
- Hydrogen and methane breath test
- Gut Microbiome Test in Dubai
- MRI abdomen and MR enterography
- CT abdomen and CT enterography
If you wish to discuss this further or would like to make an appointment, please use the booking form on this page. Expect a response within 12 business hours.