2026 Update from a UK-trained gastroenterologist in Dubai.
In my experience, active proctitis is one of the most difficult and under recognised parts of ulcerative colitis.
I say that after more than 25 years of looking after patients with IBD.
The inflamed area may be small, but the rectum is the most sensitive part of the colon. When it is inflamed, urgency, bleeding, incomplete emptying and the constant feeling that you still need to go can dominate daily life.
That is why I never judge proctitis simply by how little of the bowel appears affected. The real issue is the effect it has on the patient and whether the rectal inflammation is properly controlled.
Watch my video about proctitis, urgency and treatment
In this short video, I explain why rectal inflammation can produce such intrusive symptoms and why the discussion about local treatment should not end too early.
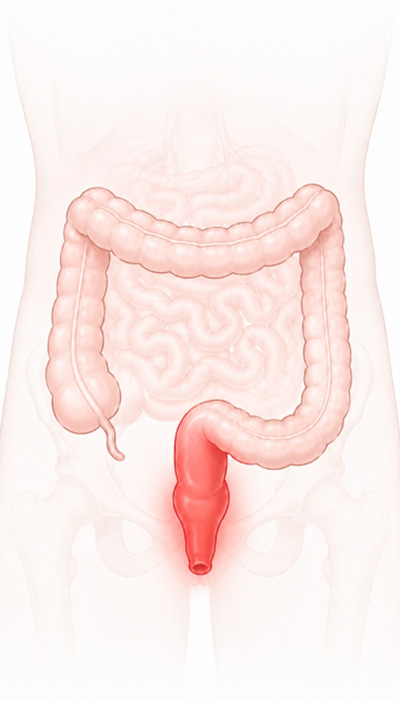
What is ulcerative proctitis?
Ulcerative proctitis is ulcerative colitis confined to the rectum.
Because the inflammation is located at the end of the bowel, local medicines such as mesalazine suppositories, rectal foam and enemas can place treatment directly onto the inflamed lining.
These treatments can be highly effective, but they can also feel awkward or difficult to use. In my view, the conversation about local treatment often ends too early, before patients understand why it matters or have had the opportunity to try a different formulation.
How common is ulcerative proctitis?
Ulcerative proctitis affects approximately 30 percent of people with ulcerative colitis, which is around 1 in 3 patients.
It is therefore not a rare form of ulcerative colitis. It represents a substantial group of people living with UC.
Why can proctitis cause severe urgency?
The rectum is designed to sense stool, pressure and the need to empty the bowel. When the rectal lining is inflamed, it may repeatedly signal that you need to go even when there is very little stool present.
Symptoms can include:
- Sudden bowel urgency
- Rectal bleeding
- Mucus
- Tenesmus, meaning the constant feeling that you still need to go
- Incomplete emptying
- Frequent attempts to open the bowel
- Difficulty confidently moving away from a toilet
The length of bowel affected does not always reflect how intrusive the symptoms will be.
In my experience, a small area of active rectal inflammation can sometimes produce more urgency and daily disruption than inflammation located higher in the colon.
Can proctitis cause constipation as well as urgency?
Yes. Some people experience constipation or difficult evacuation alongside urgency and the repeated sensation that they still need to pass stool.
This can feel contradictory. A person may feel desperate to open the bowel but pass very little because the inflamed rectum is repeatedly signalling the need to empty.
Constipation can also coexist with active inflammation and may need to be recognised and managed separately.
How is ulcerative proctitis diagnosed?
Ulcerative proctitis is diagnosed by combining the symptom history with stool tests and direct assessment of the rectum, usually by flexible sigmoidoscopy or colonoscopy with biopsies.
Assessment may include:
- A careful symptom and medication history
- Stool testing to exclude infection
- Faecal calprotectin to look for intestinal inflammation
- Flexible sigmoidoscopy or colonoscopy
- Biopsies from the rectum and colon
The extent of inflammation matters because a suppository that mainly treats the rectum may not be enough when inflammation extends further into the colon.
Read the broader ulcerative colitis symptoms and treatment guide .
Is ulcerative proctitis sometimes underestimated?
Proctitis can be treated less aggressively because it affects a smaller area, even though its effect on urgency, bleeding and daily life can remain substantial.
A recent ECCO study compared people with proctitis with those who had more extensive ulcerative colitis.
| Disease extent | Receiving advanced treatment |
|---|---|
| Ulcerative proctitis | 18.9 percent |
| More extensive ulcerative colitis | 44.3 percent |
In patient friendly terms, only around 1 in 5 people with proctitis were receiving advanced treatment, compared with nearly 1 in 2 people with more extensive ulcerative colitis.
This does not prove that everyone with proctitis should receive a biologic or another advanced medicine.
It does show that treatment intensity was much lower despite proctitis continuing to create a significant burden.
What is the usual first treatment for ulcerative proctitis?
For mild to moderately active ulcerative proctitis, local rectal 5 ASA treatment is commonly one of the first approaches discussed.
The principle is simple. The inflammation is at the end of the bowel, so the medicine is placed directly onto the inflamed lining.
Local rectal medicines may be available as:
- Suppositories
- Rectal foam
- Liquid enemas
- Other rectal formulations depending on the medicine and country
Rectal mesalazine is commonly used as a suppository or liquid enema. Rectal steroid treatment may be available as foam, an enema or another formulation.
The exact formulation depends on how far the inflammation extends, which medicine is being used and which route the patient can realistically continue.

Why local treatment matters: 5 ASA medicines act mainly through direct contact with the bowel lining. Placing the medicine onto the inflamed rectum can therefore provide a strong local anti inflammatory effect.
I have explained this in more detail in: How Salofalk, Pentasa, Asacol and other 5 ASA medicines work .
How effective are mesalazine suppositories?
In one randomised placebo controlled study, endoscopic remission after four weeks occurred in 83.8 percent of the mesalazine suppository group and 36.1 percent of the placebo group.
| Treatment | Endoscopic remission after four weeks |
|---|---|
| Mesalazine suppository | 83.8 percent |
| Placebo suppository | 36.1 percent |
Endoscopic remission means that the rectal lining looked healed or no longer actively inflamed during endoscopic assessment.
This does not mean mesalazine suppositories work for every person.
It does show that local mesalazine has meaningful evidence behind it and deserves a proper discussion before it is abandoned.
Why do people find rectal treatment difficult to continue?
Rectal treatments can feel awkward, embarrassing, uncomfortable or difficult to retain, and patients are not always given enough practical explanation or support.
A real world study of rectal mesalazine found that 71 percent of participants met the study definition of nonadherence based on prescription refill data.
This does not mean that patients did not want to improve or deliberately refused treatment.
It shows how difficult it can be to fit rectal treatment into daily life and continue it consistently.
Read the rectal mesalazine adherence research .
More recent patient research has described practical, emotional and communication barriers. Some patients felt that the difficulties of rectal treatment had not been discussed or supported properly.
Read why rectal treatment can be underused .
My view: It is not enough simply to prescribe a suppository or enema. Patients need to understand why it has been recommended, where it reaches, how to use it, what difficulties to expect and what alternatives are available.
Are suppositories, rectal foam and liquid enemas the same?
No. They differ in volume, how far they spread and how easily they can be retained.
Suppositories
Suppositories mainly treat the rectum and may be appropriate when inflammation is confined to this area.
Rectal foam
Foam may be easier for some people to retain and may spread beyond the rectum into the lower colon.
Liquid enemas
Liquid enemas generally reach further into the left side of the colon and may be useful when inflammation extends above the rectum.
One formulation being difficult to use does not mean that every type of local treatment will be unsuitable.
What should I do if I cannot tolerate a suppository or enema?
Discuss what made the treatment difficult with your gastroenterologist or IBD team before abandoning local treatment completely.
A useful discussion may include:
- Would foam be easier to retain than a liquid enema?
- Is a suppository sufficient for the area affected?
- Does the inflammation extend above the rectum?
- Am I using the medicine at the most practical time?
- How long should I continue before judging the response?
- Should local treatment be combined with oral mesalazine?
- How will we check whether the rectum has healed?
The conversation should not finish simply because the first formulation has not worked or has been difficult to use.
Can ulcerative proctitis require biologics or other advanced treatment?
Yes. Biologics or oral small molecule treatments may be considered when active proctitis continues despite appropriately used local and oral treatment.
The choice depends on disease activity, previous treatment, medical history and individual risk factors.
In my own practice, I have used advanced treatment for difficult proctitis when the disease required it.
Even when someone is receiving a biologic or another advanced medicine, I still consider whether persistent rectal inflammation may benefit from local treatment to reduce the remaining inflammatory burden.
Are mesalazine suppositories used for Crohn’s proctitis?
The strongest evidence for rectal mesalazine applies to ulcerative proctitis. Crohn’s disease affecting the rectum may require a different treatment strategy.
Crohn’s disease may produce deeper or patchier inflammation and can be associated with fissures, fistulas, abscesses, narrowing or other perianal complications.
Rectal mesalazine is not a central evidence based treatment for Crohn’s disease in the same way that it is for ulcerative proctitis.
Someone with Crohn’s disease and new rectal symptoms should discuss them with their IBD team rather than assuming the treatment will be identical to UC.
Can diet treat ulcerative proctitis?
Diet may influence symptoms, nutrition and the gut microbiome, but it does not replace proven anti inflammatory treatment for active ulcerative proctitis.
The important distinction is between:
- Food worsening symptoms
- Active inflammation causing food intolerance
- A dietary pattern influencing longer term gut health
These are not always the same thing.
Objective inflammation monitoring helps avoid blaming food for symptoms that are actually being driven by active disease.
Does the gut microbiome matter in ulcerative proctitis?
The gut microbiome is involved in ulcerative colitis biology, but an ordinary probiotic should not be viewed as a substitute for proven treatment of active rectal inflammation.
Research is moving towards specific bacterial strains, defined bacterial communities, engineered bacteria and other microbiome based approaches.
These remain separate questions from whether active proctitis needs effective local or systemic treatment now.
How do doctors check whether proctitis treatment is working?
Symptom improvement matters, but symptoms alone do not always confirm that the rectal inflammation has healed.
Monitoring may include:
- Rectal bleeding
- Urgency and bowel frequency
- Faecal calprotectin
- Blood tests
- Flexible sigmoidoscopy or colonoscopy
- Biopsies when appropriate
Calprotectin can be useful, but it should be interpreted alongside the known extent of disease, symptoms and endoscopic findings.
Persistent urgency does not always prove continuing inflammation. Constipation, infection, bowel sensitivity and other overlapping problems may also need to be considered.
What should I ask my doctor about proctitis?
- Is my inflammation confined to the rectum?
- Could active proctitis explain my urgency or incomplete emptying?
- Would a suppository, foam or liquid enema be most appropriate?
- How far does each treatment reach?
- How long should I continue the treatment?
- Should I continue local treatment after symptoms improve?
- Should local and oral mesalazine be combined?
- How will we confirm that the rectum has healed?
- What is the next option if local treatment is not enough?
- When should advanced treatment be discussed?
My view on ulcerative proctitis
In my experience, proctitis is one of the most under recognised parts of ulcerative colitis.
The affected area may be small, but the rectum is highly sensitive and the symptoms can be severe.
Local treatment has strong evidence behind it, yet it is often one of the most difficult treatments for patients to discuss and continue.
Doctors need to explain it better, acknowledge the practical difficulties and avoid ending the conversation after one formulation has not worked or has not suited the patient.
The objective is not simply to prescribe a suppository or enema.
It is to find a treatment route the patient can use and to get the rectal inflammation properly controlled.
Research used in this article
- How common ulcerative proctitis is and how clinicians approach it
- ECCO research on proctitis burden and advanced treatment use
- Randomised study of mesalazine suppositories
- Real world research on continuing rectal mesalazine
- Patient experiences and barriers to rectal treatment
- Current clinical guidance for ulcerative colitis treatment
Important information
This article is for general education only. It does not provide a diagnosis, an individual treatment recommendation or an electronic consultation.
Rectal bleeding, severe pain, fever, increasing bowel frequency, dehydration or rapidly worsening symptoms require prompt medical assessment.
Speak to your own gastroenterologist or IBD team before starting, stopping or changing treatment.
If you wish to discuss this further or would like to make an appointment, please use the booking form on this page. A member of our team will contact you within 12 business hours.