By Dr Pranab Gyawali, Consultant Gastroenterologist (UK-trained) in Dubai
Is taking a probiotic automatically helping your gut?
No. A probiotic's effect depends on the organism, the strain, the reason it is being used, the diet, the surrounding microbiome and the person taking it.
I am Dr Pranab Gyawali, a consultant gastroenterologist with more than 25 years' clinical experience. In recent years, a large part of my educational and clinical interest has been in the gut microbiome: not as a wellness slogan, but as something that may eventually help us understand why diet, inflammation, the mucus barrier and microbes interact so differently from one person to another.
That is why I made this short video. I am not against probiotics. But I am against the lazy idea that anything labelled as "good bacteria" must automatically be good for every gut.
Many people with Crohn's disease, ulcerative colitis, IBS or general gut symptoms have already tried several probiotic products. When I moved to Dubai roughly four years ago, I counted nearly 80 probiotic products on the market, all making slightly different gut-health promises. That was not a formal market audit. It was simply what patients were already facing: too many claims, and not enough precision.
If a probiotic has been prescribed or recommended for a specific clinical reason, do not stop it because of this article. Discuss it with the clinician or dietitian overseeing your care. The issue here is indiscriminate self-selection and overinterpretation of broad probiotic marketing.
Watch the short video
This page is based on my short VLOG on Akkermansia, probiotics and why the gut environment matters.
If you prefer to watch first, start with the video. In less than two minutes, I explain why taking another probiotic does not automatically mean you are helping your gut, and why Akkermansia is a good example of the problem with simple "good bacteria" thinking.
Why Akkermansia is a useful example
Akkermansia muciniphila is a normal gut bacterium that lives close to the mucus layer of the bowel. It is often discussed as a beneficial or next-generation probiotic organism because it has been associated in research with gut-barrier and metabolic health.
But association is not the same as treatment proof.
A bacterium associated with health is not automatically a bacterium proven to restore health when taken as a supplement. Its effect may depend on the diet, the other microbes around it and the condition of the bowel.
That is what makes Akkermansia useful for this discussion. It shows why the question should not be, "Is this bacterium good or bad?" The better question is, "What is this bacterium doing in this particular gut environment?"
What the mouse study showed
A 2024 study in Molecular Systems Biology looked at Akkermansia in a controlled mouse experiment.
The researchers used germ-free or gnotobiotic mice and introduced defined synthetic gut microbial communities. These were not ordinary mice with a natural mixed microbiome. They were mice colonised with specific combinations of bacteria, including communities with or without Akkermansia.
The researchers compared a fibre-rich diet with fibre deprivation and then exposed the mice to Citrobacter rodentium, a pathogen used in mouse models of intestinal infection.
The result was not a simple "Akkermansia is good" or "Akkermansia is bad" result.
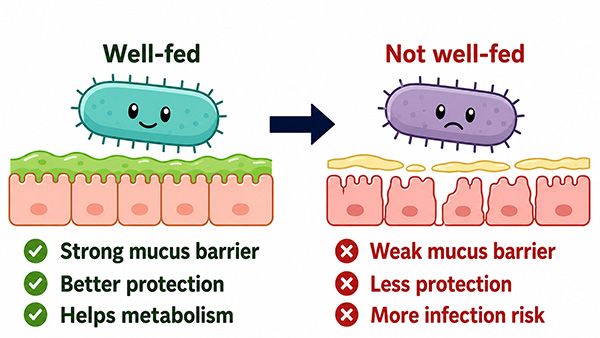
On a fibre-rich diet, the Akkermansia-containing community was associated with lower pathogen burden and greater resistance. But during fibre deprivation, within a disrupted synthetic microbial community, the presence of Akkermansia was linked with a more penetrable mucus layer and greater susceptibility to infection.
That is the key lesson: the same commensal bacterium had different net effects in different dietary and microbial contexts.
This was not a human trial. It was not a study of people with Crohn's disease or ulcerative colitis taking Akkermansia supplements. It does not prove that Akkermansia supplements damage the human bowel. It also does not mean Akkermansia "turned pathogenic".
Akkermansia is naturally a mucin specialist. The experiment changed the wider diet-microbiome ecosystem. The practical lesson is context dependence, not fear.
Diet, fibre and the gut environment
Often, diet is the better place to start than another capsule. But even that needs nuance.
Fibre can shape the microbiome, microbial metabolism and the mucus barrier. A probiotic does not enter an empty laboratory system; it enters a living bowel with an existing diet, immune state, microbial community and disease context.
For many people, improving dietary diversity and fibre quality may matter more than buying another probiotic. But this should not become a blanket instruction that every person with IBD must increase fibre.
Some patients with Crohn's disease or ulcerative colitis cannot tolerate unrestricted fibre, especially during severe active symptoms, obstructive symptoms, known stricturing Crohn's disease or specific medically supervised dietary periods.
So the more accurate message is this: dietary diversity and fibre should be individualised according to disease activity, bowel anatomy and tolerance.
The point is not that patients are responsible for damaging their bowel if they cannot tolerate fibre. The point is that diet and microbial context influence how bacteria behave.
What this means before buying a probiotic
"Good bacteria" is too vague to guide a decision.
Before buying a probiotic, I would want to know the organism, the strain, the dose, the preparation, the condition it was studied for and whether the evidence comes from humans, animals or laboratory models. A probiotic studied for antibiotic-associated diarrhoea is not automatically a probiotic for Crohn's disease. A bacterium associated with metabolic health is not automatically a treatment for gut inflammation.
This is particularly relevant in Crohn's disease and ulcerative colitis. Standard probiotics may have a role in selected situations, especially for some patients with ulcerative colitis or pouch-related problems, but they are not a replacement for proper assessment, inflammation monitoring or established IBD treatment when these are needed.
For a broader discussion of how newer microbiome therapies differ from ordinary probiotic supplements, see my page on next-generation probiotics for Crohn's disease and ulcerative colitis.
Why I am still interested in smarter microbial therapies
I am following next-generation probiotic and live-biotherapeutic approaches closely because they are different from ordinary broad gut-health products.
The interesting direction is not simply to add more bacteria. It is to use defined strains, defined bacterial communities or engineered bacteria to produce specific biological effects, and then test those effects properly.
For example, MH002 is a six-strain live biotherapeutic being studied in ulcerative colitis. It is a useful example because it is not simply a shop-bought probiotic; it is a defined microbial consortium being tested with clinical outcomes and safety monitoring.
Engineered E. coli Nissle 1917 TTR is another approach, designed around a specific inflammatory environment. MB310 is a defined microbial treatment studied in ulcerative colitis. SER-603 is another investigational microbiome-based approach.
These are not established or approved IBD treatments. They are examples of how the field is trying to move from vague probiotic claims towards more specific, measurable and clinically tested microbial therapies.
That is a very different conversation from buying a product because the label says it contains "good bacteria".
My view
The Akkermansia study is not a reason to be frightened of probiotics.
It is a reason to be more discerning.
If a probiotic has been recommended for a specific reason, discuss it with your clinical team rather than stopping it suddenly. But if you are choosing products for yourself based on broad gut-health claims, it is worth pausing.
Ask what the product is supposed to do, whether that exact organism or strain has been tested for your situation, and whether your diet and gut environment are being considered at the same time.
The future of microbiome treatment may be genuinely useful for Crohn's disease, ulcerative colitis and wider gut health. But we need organism-specific, strain-specific and condition-specific evidence, not simply the words "good bacteria" on a box.
A bacterium associated with health is not automatically a bacterium proven to restore health.
Short FAQ
Does this prove Akkermansia supplements are harmful?
No. The 2024 study was a controlled mouse experiment using defined synthetic microbial communities and an intestinal infection model. It was not a human supplement trial.
Should everyone with IBD increase fibre?
No. Fibre advice must be individualised in Crohn's disease and ulcerative colitis, especially during severe symptoms, stricturing disease or obstructive symptoms.
What is the main takeaway before buying a probiotic?
Do not judge a probiotic by the phrase "good bacteria". Ask which organism and strain it contains, what condition it was studied for and whether the evidence applies to your gut problem.
Research used in this article
Diet-driven differential response of Akkermansia muciniphila modulates pathogen susceptibility. Molecular Systems Biology. 2024;20:596-625.
This was a controlled mouse study using defined synthetic microbial communities. It should not be interpreted as a human trial of Akkermansia supplements or as proof of harm in Crohn's disease or ulcerative colitis.
Recommended related reading
For the wider microbiome and diet context
- Gut microbiome in Crohn's disease and ulcerative colitis
- Diet, microbiome and IBD: how the right bacteria calm gut inflammation
- Ultra-processed foods and gut microbiome health
- 4 science-backed tips to support your gut barrier if you have Crohn's or UC
For probiotics and live biotherapeutics
- Next-generation probiotics for Crohn's disease and ulcerative colitis
- Next generation probiotic MH002 for ulcerative colitis
- Probiotics for ulcerative colitis: what actually works?
- E. coli Nissle 1917 probiotic for ulcerative colitis
- Engineered probiotic for ulcerative colitis 2026
If you wish to discuss this further or would like to make an appointment, please use the booking form on this page. A member of our team will contact you within 12 business hours.