2026 Update from a UK-trained gastroenterologist in Dubai.
Two new studies offer clues about predicting the future course of inflammatory bowel disease.
Why predicting the course of IBD matters
One of the first questions people ask me after being diagnosed with Crohn’s disease or ulcerative colitis is:
“How severe is this going to become?”
I have looked after people with inflammatory bowel disease (IBD) for more than 25 years. There are certainly patterns that an experienced clinician begins to recognise.
But I also have to be honest: there have been patients whose disease behaved differently from what I initially expected. That is why improving prediction matters—not as an academic exercise, but because it may eventually help us treat a higher-risk patient earlier while avoiding unnecessary escalation in someone whose disease may remain relatively mild.
Can doctors predict how severe IBD will become?
Doctors can estimate the risk of a more severe Crohn’s disease or ulcerative colitis course, but we cannot yet predict an individual patient’s future with certainty. We currently use disease location and extent, ulcer severity, complications, endoscopy, imaging, blood tests and stool calprotectin. Two recent studies suggest that microbiome patterns, anti-IL-10 antibodies and genetics may eventually add further information.
Key findings at a glance
| Area | What was assessed | Main finding |
|---|---|---|
| Current clinical assessment | Disease extent, ulcers, fistulas, strictures, imaging, CRP and stool calprotectin | Useful for estimating risk, but not a precise individual forecast |
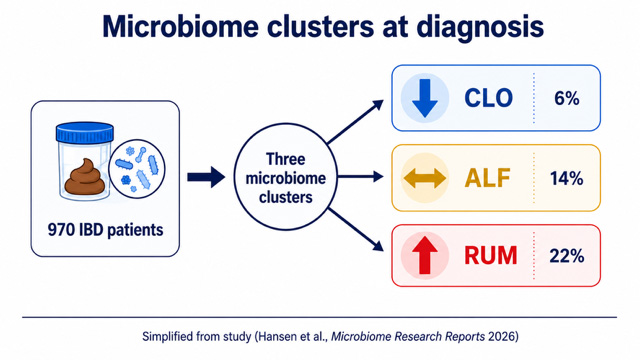
| Norwegian microbiome study | Stool microbiome from 970 newly diagnosed IBD patients | Severe one-year course in 6%, 14% and 22% across three microbiome clusters |
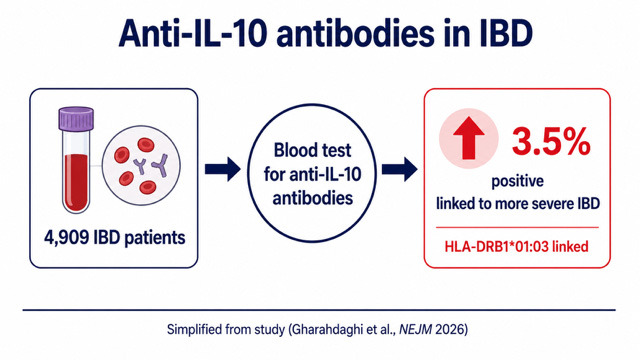
| Oxford-led anti-IL-10 study | Blood samples from 4,909 IBD patients | Anti-IL-10 antibodies in 3.5%, strongly associated with HLA-DRB1*01:03 |
| Clinical status | Research-stage prediction tools | Neither test is currently part of routine IBD risk assessment |
Watch the video
How do gastroenterologists currently estimate IBD risk?
At diagnosis, we assess how much of the bowel is involved, how severe the inflammation and ulcers appear, and whether Crohn’s disease has already caused narrowing, penetrating disease, fistulas, abscesses or perianal complications.
We also use blood markers such as CRP, albumin and haemoglobin, alongside stool calprotectin, endoscopy and imaging. The early need for steroids, admission to hospital or rapid treatment escalation can also signal a higher-risk course.
These factors influence decisions about monitoring and whether earlier biologic or advanced IBD treatment may be appropriate. They are valuable, but they are still imperfect predictors.
A large prospective study has also reinforced the value of stool calprotectin in predicting future inflammatory flares: diet, calprotectin and flare risk in Crohn’s disease and ulcerative colitis .
Study 1: Can microbiome patterns predict a severe IBD course?
A Norwegian-led team analysed stool samples from 970 people newly diagnosed with IBD in the population-based IBSEN III programme.
Instead of focusing on one supposedly helpful or harmful bacterium, the researchers used computer modelling to examine the microbiome as an organised community. The analysis identified three clusters: CLO, ALF and RUM.
In the first year, the proportion meeting the study definition of a severe disease course was:
- CLO cluster: 6%
- ALF cluster: 14%
- RUM cluster: 22%
Read the Norwegian microbiome study
What did “severe disease course” mean?
This was not simply another term for having symptoms or one flare. The definition included outcomes such as IBD-related hospitalisation or surgery, repeated corticosteroid courses, progression through several biologic treatments and, in Crohn’s disease, new strictures, fistulas or abscesses.
The microbiome clusters performed approximately as well as stool calprotectin in the prediction model. More importantly, combining microbiome-cluster information with calprotectin improved the model further.
How useful is this study clinically?
This is a promising direction, but it is not yet a clinical test. The result came from one Norwegian cohort, used baseline microbiome samples and has not yet been independently validated across different populations.
The study does not justify buying a commercial microbiome report to predict whether an individual patient’s IBD will become severe. What it adds is evidence that whole microbial patterns may contain clinically useful information when combined with established markers.
For the wider clinical context, read: the gut microbiome in Crohn’s disease and ulcerative colitis .
Study 2: Anti-IL-10 antibodies and HLA-DRB1*01:03
An Oxford-led collaboration analysed blood from 4,909 patients with Crohn’s disease or ulcerative colitis. Neutralising antibodies against interleukin-10, or IL-10, were found in 173 patients—approximately 3.5%.
IL-10 helps restrain inflammatory immune responses. I describe it to patients as one part of the immune system’s natural braking mechanism. In this subgroup, antibodies appeared to block that brake.
These antibodies were strongly associated with an inherited genetic marker called HLA-DRB1*01:03.
Read the Oxford anti-IL-10 antibody study
Read the HLA-DRB1*01:03 genetic study
Does this provide a new IBD prediction blood test?
Not yet. Anti-IL-10 antibody testing and HLA-DRB1*01:03 testing are not currently routine prognostic investigations for most patients with IBD.
The 3.5% result also does not mean that every antibody-positive patient will inevitably develop severe disease. The study identifies a biologically distinct subgroup and a plausible mechanism, not a guaranteed outcome for an individual patient.
This research is important because it connects a genetic marker associated with severe IBD to a specific immune abnormality that may eventually be measurable and potentially targetable.
What do these studies add to IBD prediction?
These studies approach the same clinical problem from different directions.
The Norwegian study asks whether the organisation of the gut microbiome contains information about where the disease may be heading. The Oxford-led work identifies an immune abnormality linked to an inherited genetic marker associated with a more severe phenotype.
My view is that no single marker will provide the entire answer. Better prediction will probably require several forms of information to be interpreted together:
- clinical disease pattern and previous behaviour
- endoscopy and imaging
- blood tests and stool calprotectin
- genetic markers
- immune proteins and antibodies
- microbiome patterns
- response to treatment over time
This is related to the wider development of multi-omics prediction in Crohn’s disease and ulcerative colitis , where several biological layers are analysed together rather than relying on one isolated result.
How could AI improve prediction in Crohn’s disease and ulcerative colitis?
The difficulty is increasingly not collecting data. It is making sense of the volume and complexity of that data.
A microbiome dataset alone can contain information from hundreds or thousands of organisms. Genetics, endoscopy, imaging, immune markers and repeated blood and stool results add many more variables.
Machine learning and artificial intelligence may help identify combinations that are difficult to recognise reliably by eye alone. The Norwegian research programme is already exploring AI-assisted microbial precision medicine.
This does not mean allowing a computer to make treatment decisions independently. The more credible future is AI supporting the gastroenterologist by integrating complex information while the clinician remains responsible for interpretation and decision-making with the patient.
Read more about AI and machine learning in IBD treatment prediction .
What does this mean for patients today?
These studies do not currently change routine Crohn’s disease or ulcerative colitis treatment. Established clinical assessment, endoscopy, imaging, blood tests and stool calprotectin remain more useful today than commercial microbiome or genetic reports.
Useful questions to ask your IBD team include:
- Which features make my disease appear higher or lower risk?
- How extensive and severe was the inflammation at diagnosis?
- How will we confirm that inflammation is genuinely controlled?
- What finding would make us intensify or change treatment?
The choice of treatment already involves several clinical and practical factors. Read more about how gastroenterologists choose a biologic for Crohn’s disease and ulcerative colitis .
My current view
After more than 25 years in IBD practice, I have learned that experience helps us recognise important patterns—but prediction remains imperfect.
What makes me optimistic is that several useful types of data are emerging at the same time. We are learning more from microbiome research, genetics, immune markers, imaging and molecular studies. At the same time, machine learning and AI are becoming better at analysing complex information.
Therefore, better prediction may not come from one dramatic breakthrough or one perfect test. It may come from bringing several imperfect but useful signals together.
That now feels much more achievable than it did even a few years ago, and it is an area I will continue to follow closely.
Frequently asked questions
Can doctors predict how severe Crohn’s disease or ulcerative colitis will become?
Doctors can estimate risk using disease extent, ulcer severity, complications, imaging, endoscopy, blood tests, stool calprotectin and early disease behaviour. No current test can predict an individual patient’s course with certainty.
Can a microbiome stool test currently predict severe IBD?
No. The Norwegian study identified research-level microbiome clusters associated with different outcomes. The findings require independent validation before they can become a clinical test.
What is HLA-DRB1*01:03?
HLA-DRB1*01:03 is an inherited immune-system genetic marker associated with both Crohn’s disease and ulcerative colitis and, in recent large-scale research, with a more severe disease phenotype.
What are anti-IL-10 antibodies?
These are antibodies that neutralise IL-10, a protein that normally helps regulate inflammation. They were identified in approximately 3.5% of patients in the Oxford-led study and were strongly associated with HLA-DRB1*01:03.
Will AI decide which IBD treatment I should receive?
AI may eventually help specialists combine complex clinical, genetic, immune and microbiome information. It should support, rather than replace, specialist clinical judgement and decisions made with the patient.