It can be incredibly frustrating when a biologic works brilliantly and then seems to stop.
I have been treating patients with biologics since infliximab first became established in IBD nearly 20 years ago, and I have seen this situation many times in both UK and international practice.
The important point is this: a biologic appearing to stop working does not automatically mean complete treatment failure.
Watch my explanation
In this short video, I explain why a biologic may appear to stop working and why the first step is to confirm whether inflammation is genuinely active.
The short answer
When a biologic appears to stop working, the first step is to confirm whether there is genuinely active inflammation. If there is, three common possibilities we consider are inadequate drug exposure, anti-drug antibodies with some biologics, or active inflammation that is no longer sufficiently controlled by the current treatment mechanism.
First, is there really active inflammation?
This question comes before drug levels, antibodies or switching treatment.
Diarrhoea, urgency, abdominal pain, bloating and fatigue can return even when Crohn's disease or ulcerative colitis inflammation is not the main problem. Symptoms can also return because of infection, IBS-type overlap, bile acid diarrhoea, constipation or a structural complication such as a stricture.
Your gastroenterologist may therefore look at symptoms together with blood tests, faecal (fecal) calprotectin, stool tests, imaging, intestinal ultrasound where available, or endoscopy.
This is also why the concept of deep remission in Crohn's disease and ulcerative colitis matters. In IBD, feeling better is important, but doctors also need to know whether inflammation is actually controlled.
Why might the drug level be too low?
If active inflammation is confirmed, one possibility is inadequate drug exposure.
Biologics need to remain at a sufficient level in the body to keep inflammation under control. Some patients clear the medicine faster than expected. This can happen with a high inflammatory burden, low albumin, protein loss through the inflamed bowel, body size, or individual differences in how the medicine is handled.
The result may be that the biologic works for part of the dosing interval but is no longer enough before the next dose is due.
Drug-level testing is best established for anti-TNF medicines, especially infliximab and adalimumab. It is not equally available, validated or clinically useful for every biologic.
Could anti-drug antibodies be interfering?
Another possibility is anti-drug antibodies.
Biologics are protein medicines. In some patients, the immune system recognises the medicine as foreign and produces antibodies against it. These antibodies may reduce the amount of active medicine in the body or reduce how well the medicine works.
Again, this is most established for anti-TNF medicines such as infliximab and adalimumab. The result also needs interpretation. A low or temporary antibody result is not the same as a high, persistent antibody level with very little drug remaining.
Why might the current biologic mechanism no longer be enough?
Sometimes the drug level is adequate and there are no significant antibodies, but inflammation remains active. This may mean that the treatment mechanism is no longer sufficient to control the inflammation, although routine clinical tests cannot usually identify a precise pathway switch.
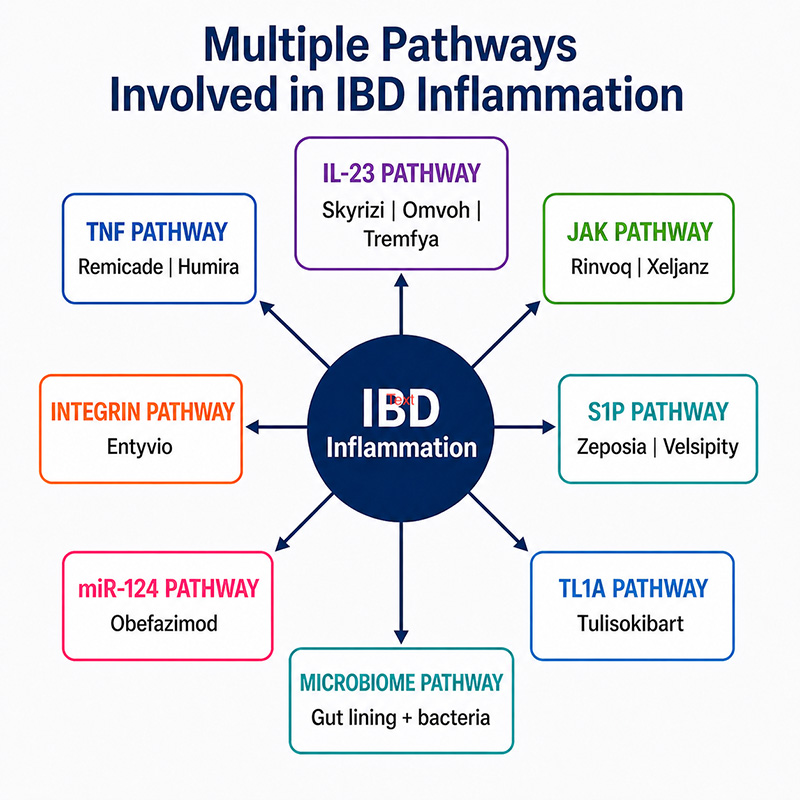
Crohn's disease and ulcerative colitis can involve several overlapping inflammatory pathways. Biologics may target TNF, integrins or interleukins. Other pathways, including JAK signalling, S1P, TL1A and miR-124, help illustrate why IBD inflammation is biologically complex.
The practical point is not to memorise every pathway. It is that a biologic that was once enough may not always remain enough.
For more background, see why biologics work for some IBD patients but not others and how biologics work in Crohn's disease and ulcerative colitis.
What might your gastroenterologist consider next?
The next step depends on what the assessment shows.
If there is no clear active inflammation, it may be safer to look for another explanation for symptoms rather than abandon a biologic that is still controlling IBD.
If inflammation is active and the drug level is low, treatment optimisation may be considered for selected biologics. If antibodies are important, a change in strategy may be needed. If drug levels are adequate and inflammation remains active, a biologic with a different mechanism may be discussed.
Treatment decisions depend on the biologic being used, disease location and severity, previous treatment response, complications, safety history, other medical conditions and local availability.
This is why treatment selection is individual. I have explained this further in how we choose a biologic in IBD and on the main biologics for IBD page.
Do not stop, increase or switch a biologic without discussing it with your gastroenterologist or IBD team.
My view
In my view, "the biologic has failed" is often too blunt. The more useful question is why control has been lost. Confirming inflammation, understanding drug exposure and recognising when a different treatment mechanism may be needed leads to a far more rational next decision.
I know how frustrating it can feel when a treatment that worked well appears to stop. But this should be the beginning of working out why, not simply the end of that treatment discussion.
If you wish to discuss this further or would like to make an appointment, please use the booking form on this page.
Frequently asked questions
What does biologic loss of response mean?
It means a biologic that previously controlled Crohn's disease or ulcerative colitis is no longer controlling inflammation well enough. Symptoms alone are not enough to prove this.
Does returning diarrhoea mean my biologic has failed?
No. Diarrhoea can return because of active inflammation, but also because of infection, IBS-type overlap, bile acid diarrhoea, constipation or other causes.
Can drug levels and antibodies be checked for every biologic?
Not in the same way. Drug-level and antibody testing are best established for anti-TNF medicines, especially infliximab and adalimumab. Testing is not equally available or useful for every biologic.
Can a biologic work again after treatment optimisation?
Sometimes. If the main problem is inadequate drug exposure, optimisation may help selected patients. This depends on the biologic, test results and clinical context.
Research used in this article
- ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial diagnosis, monitoring of known IBD, detection of complications
- Appropriate Therapeutic Drug Monitoring of Biologic Agents for Patients With Inflammatory Bowel Diseases
The evidence for drug levels and anti-drug antibodies is strongest for anti-TNF medicines. Some principles apply more broadly to biologic loss of response, but testing and interpretation differ by biologic. A precise pathway switch usually cannot be identified by routine clinical tests.
Recommended VLOGs and guides
- Why biologics work for some IBD patients but not others
- How biologics work in Crohn's disease and ulcerative colitis
- How we choose a biologic in IBD
- Biologics for IBD
- Deep remission in Crohn's disease and ulcerative colitis
Important information
This article is for general education only. It does not provide a diagnosis, an individual treatment recommendation or an electronic consultation.
Do not stop, delay, increase or change a biologic without speaking to your own gastroenterologist or IBD team.
New or worsening bleeding, fever, severe abdominal pain, dehydration, rapid weight loss or rapidly worsening bowel symptoms require prompt medical assessment.