By Dr Pranab Gyawali, Consultant Gastroenterologist (UK-trained) in Dubai
A patient asked me about this just this week. Their faecal calprotectin was very high, but their CRP blood test was completely normal.
That can feel contradictory. If one inflammation test is high, why is the other one normal?
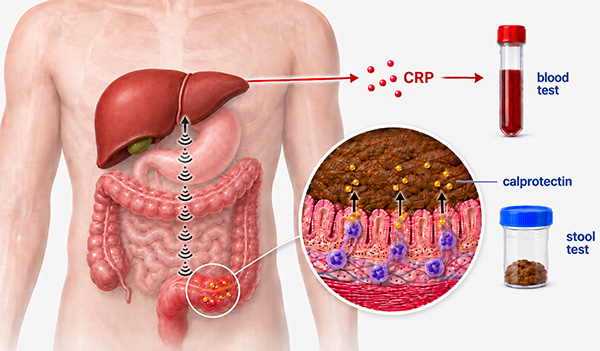
The short answer is this: faecal calprotectin and CRP measure different parts of the inflammatory response. Calprotectin reflects inflammatory-cell activity directly in the bowel and is measured in stool. CRP is produced by the liver when inflammatory signals from the body are strong enough to trigger a wider response in the blood.
So yes, you can have active bowel inflammation from Crohn's disease or ulcerative colitis with a high calprotectin and a normal CRP. A normal CRP does not automatically rule out active inflammatory bowel disease.
If you prefer to watch the short video first, you can watch it here:
Why can calprotectin be high when CRP is normal?
Calprotectin comes mainly from neutrophils, a type of white blood cell involved in inflammation. When the lining of the bowel is inflamed, these cells move into the bowel wall and bowel lumen. Calprotectin is then released and can be detected in the stool.
This is why faecal, or fecal, calprotectin is useful in IBD. It gives a bowel-focused signal. It is not perfect, but it often tells us more about inflammation in the gut than symptoms alone.
CRP works differently. CRP is made mainly by the liver as part of the acute-phase response. For CRP to rise, inflammatory signals need to travel beyond the bowel and stimulate the liver strongly enough to increase CRP production.
Sometimes that happens. Sometimes it does not.
Does a normal CRP rule out active IBD?
No. This is the point I most want patients to understand.
A normal CRP can be reassuring in the right context, but it does not overrule a clearly raised calprotectin. The two tests are measuring different smoke signals.
Some people with Crohn's disease produce a strong CRP response when their disease is active. Other people produce very little CRP, even when there is bowel inflammation. In ulcerative colitis, CRP can be modest or even absent despite active inflammation.
That is why your gastroenterology team will usually interpret CRP alongside symptoms, faecal calprotectin, stool infection tests where needed, blood count, albumin, imaging, intestinal ultrasound where available, or endoscopy.
Can calprotectin be high for reasons other than IBD?
Yes. A high calprotectin means there is a bowel inflammation signal. It does not automatically tell us the cause.
Calprotectin can rise with active Crohn's disease or ulcerative colitis, but it may also rise with bowel infections, some medicines such as non-steroidal anti-inflammatory drugs, and other conditions that irritate or inflame the bowel.
This is why a single result should not be interpreted in isolation. The level matters, but so does the story around it: symptoms, recent infections, medication use, previous IBD history, colonoscopy findings and whether the result is rising, falling or persistent.
What should you do with a high calprotectin and normal CRP?
If the calprotectin is unexpectedly high, I would not ignore it just because CRP is normal.
The next step depends on the person. In someone with known IBD, the question is whether this reflects active Crohn's disease or ulcerative colitis, infection, medication effect, or another bowel problem. In someone without a diagnosis of IBD, the result may need repeat testing, infection exclusion, or further assessment depending on symptoms and the actual level.
Very high values, especially if they persist or fit with symptoms such as diarrhoea, bleeding, weight loss, pain or night-time symptoms, deserve proper review.
That does not mean every high calprotectin requires urgent colonoscopy. It means the result needs context.
Where might newer stool markers fit in?
Calprotectin has been an important test in IBD. I remember how much it changed clinical practice when it first arrived in the NHS nearly 18 years ago. It gave us a non-invasive way to track bowel inflammation without relying only on symptoms or repeated invasive tests.
But calprotectin is still a broad inflammation marker. It does not always distinguish IBD inflammation from other causes of bowel inflammation.
That is why I am watching the next generation of stool markers closely, including Granzyme A.
The cautious way to describe Granzyme A is this: it is a potential new stool marker for IBD. Early research suggests it may give a more specific signal of immune activity in the bowel. It is not a replacement for calprotectin in routine practice today, and it should not be treated as a commercially available answer for every patient.
Dr Pranab's current view
When I see high calprotectin with normal CRP, I do not treat the normal CRP as the final answer.
I ask what the calprotectin is telling us about the bowel, whether the result fits the symptoms, whether infection or medicines could explain it, and whether we need objective assessment of the bowel.
The practical message is simple: a normal CRP is useful information, but it does not cancel out a very high calprotectin.
Frequently asked questions
Can calprotectin be high if my blood tests are normal?
Yes. Calprotectin can be high because it reflects inflammation in the bowel itself. Blood tests, including CRP, may remain normal in some people with active bowel inflammation.
Does a normal CRP mean my Crohn's disease or ulcerative colitis is inactive?
Not always. Some people have active IBD with a normal CRP. Your doctor may need to look at calprotectin, symptoms, stool tests, imaging or endoscopy before deciding whether inflammation is active.
Is calprotectin specific for IBD?
No. Calprotectin is a bowel inflammation marker, but it is not specific to Crohn's disease or ulcerative colitis. Infection, medicines such as NSAIDs and other bowel conditions can also raise it.
Should I repeat a high calprotectin test?
Sometimes. Repeat testing can be useful, especially if the result is borderline or there is a possible temporary cause. Very high or persistent results usually need clinical interpretation rather than reassurance from a normal CRP alone.
What is Granzyme A?
Granzyme A is being studied as a potential new stool marker for IBD. It may eventually help identify IBD-related immune activity more specifically, but it is not currently a routine replacement for calprotectin.
Research used in this article
For background on faecal calprotectin, see Fecal calprotectin in inflammatory bowel disease. For CRP in IBD, see C-reactive protein as a marker for inflammatory bowel disease. For the emerging Granzyme A research, see A chemiluminescence assay targeting granzyme A activity for monitoring inflammatory bowel disease.
Recommended VLOGs and guides
If you are trying to understand where this result fits, these related pages may help:
- Granzyme A and next-generation stool testing in IBD
- Can smartwatches predict IBD flares?
- Diet, calprotectin and the PREdiCCt flare-prediction study
- Bread, ultra-processed grains and IBD
- Why a biologic may stop working in IBD
- Biologics for Crohn's disease and ulcerative colitis
This article is for general education and should not replace personal medical advice. If your calprotectin is unexpectedly high, persistently high, or high alongside worrying symptoms, discuss the result with your own gastroenterology team.
If you wish to discuss this further or would like to make an appointment, please use the booking form on this page. A member of our team will contact you within 12 business hours.