By Dr Pranab Gyawali, Consultant Gastroenterologist (UK-trained) in Dubai
I am Dr Pranab Gyawali, a consultant gastroenterologist with more than 25 years of experience looking after patients with Crohn’s disease and ulcerative colitis.
In this VLOG, I describe how difficult and distressing Crohn’s fistulas and perianal fistulas can be, and why the new FUZION Tremfya, also called guselkumab, data caught my attention.
Crohn’s fistulas are not just a medical term. For many patients, they can mean pain, discharge, abscesses, setons, embarrassment, repeated procedures and fear of further surgery.
For people who want to look at the presentation behind this discussion, the FUZION Phase 3 DDW 2026 presentation can be viewed here.
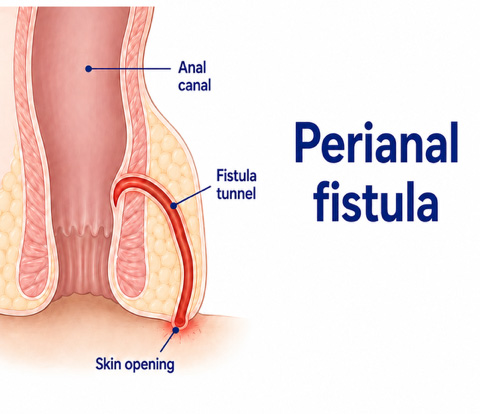
A fistula is an abnormal tunnel. In Crohn’s disease, inflammation can go through the full thickness of the bowel wall. Around the back passage, this can create a tunnel from the anal canal or rectum to the skin.
This is called a perianal fistula.
Perianal fistulas are important because they are painful, difficult to treat and often need both medical and surgical management. AGA has described Crohn’s perianal fistula as affecting about 25% of Crohn’s disease patients.
Crohn’s fistulas can affect quality of life far beyond bowel symptoms.
| Problem | What it may mean for patients |
|---|---|
| Pain | Difficulty sitting, walking or sleeping |
| Discharge | Ongoing leakage, staining and discomfort |
| Abscesses | Infection, fever and emergency drainage |
| Setons | A surgical thread used to keep the tract draining safely |
| Repeated procedures | MRI scans, drainage, surgery and follow up |
| Emotional impact | Embarrassment, anxiety and loss of confidence |
This is why I always say perianal Crohn’s needs a strategy, not just a prescription.
Before biologics, treatment was much more limited. Many patients had repeated courses of antibiotics, drainage of abscesses, seton placement and surgery. These treatments were important, and still are, but they often did not control the underlying Crohn’s inflammation well enough.
When infliximab, Remicade, became available, it changed the way many of us thought about fistulising Crohn’s disease.
I remember patients in London in the early biologic era who could barely sit down because of severe perianal Crohn’s. Some had painful fistulas, discharge, setons and colonic Crohn’s disease at the same time. When infliximab worked, the change could be dramatic. Pain improved, discharge reduced and some patients returned to a much more normal life.
That is why infliximab became the landmark biologic in Crohn’s fistula care.
The FUZION study looked at guselkumab, also known by the brand name Tremfya, in adults with active perianal fistulising Crohn’s disease.
Guselkumab is an IL 23 inhibitor. This is a different biologic pathway from infliximab, which is an anti TNF drug.
In my view, this data matters because more than 20 years after infliximab changed fistula care, we still have surprisingly few large, dedicated randomized trials focused specifically on active perianal fistulising Crohn’s disease.
This does not mean other biologics have no role. Adalimumab, Humira, ustekinumab, Stelara, and vedolizumab, Entyvio, all have supportive data and are used in clinical practice.
But FUZION feels different because it is a large, Phase 3, randomized, double blind, placebo controlled study built specifically around this difficult Crohn’s phenotype.
At week 24, which is about six months, Tremfya, guselkumab, achieved higher combined fistula remission than placebo.
| FUZION Phase 3 result | What it showed |
|---|---|
| Study population | Adults with active perianal fistulising Crohn’s disease |
| Number randomized | 286 patients |
| Treatment | Tremfya, guselkumab, versus placebo |
| Time point | Week 24, about six months |
| Main endpoint | Combined fistula remission |
| Guselkumab result | About 27 to 28% |
| Placebo result | About 10% |
| Key point | Nearly three times higher remission than placebo |
This is encouraging.
But it is also realistic. Around two thirds of patients still had not achieved complete combined fistula remission by six months. So this is not a cure for everyone. It is progress in a very difficult area.
In my opinion, this data is likely to influence future guideline discussions.
That does not mean Tremfya automatically replaces existing treatments. Infliximab remains very important. Adalimumab, ustekinumab, vedolizumab, surgery, antibiotics, setons and multidisciplinary care all still have roles.
But I do think FUZION may position Tremfya, guselkumab, more strongly in fistulising Crohn’s disease, particularly after infliximab or in patients where a different pathway is needed.
No.
Perianal Crohn’s disease is complex. The right treatment depends on several clinical factors.
| Clinical factor | Why it matters |
|---|---|
| Is there an abscess? | Abscesses usually need drainage |
| Is there a seton? | Setons may be needed to control sepsis and drainage |
| Is the rectum inflamed? | Rectal inflammation makes fistulas harder to heal |
| Has MRI mapped the fistula? | MRI helps define the tract and hidden collections |
| Has anti TNF treatment already been used? | Previous response or failure affects sequencing |
| Is there active luminal Crohn’s? | Bowel inflammation must also be controlled |
This is why perianal fistulising Crohn’s usually needs both a gastroenterologist and a colorectal surgeon.
If you have Crohn’s fistulas, this is worth knowing about.
It does not mean you should stop your current treatment or ask to switch immediately. But it does mean the treatment landscape is moving.
The most important message is that Crohn’s fistulas need a planned approach.
| Step | Why it matters |
|---|---|
| MRI pelvis | Maps the fistula and checks for abscess |
| Surgical review | Looks at drainage, seton and sepsis control |
| Biologic strategy | Chooses the right immune pathway |
| Monitoring | Tracks drainage, pain, calprotectin and imaging |
| Long term plan | Prevents repeated flares, abscesses and surgery |
What is a Crohn’s fistula?
A Crohn’s fistula is an abnormal tunnel caused by deep inflammation. Around the back passage, it can connect the anal canal or rectum to the skin. This is called a perianal fistula.
How common are perianal fistulas in Crohn’s disease?
Perianal fistulas can affect about 25% of patients with Crohn’s disease, although estimates vary depending on the population studied and how fistulas are defined.
What is Tremfya or guselkumab?
Tremfya is the brand name for guselkumab, a biologic medicine that targets IL 23, an inflammatory pathway involved in Crohn’s disease and ulcerative colitis.
What is the FUZION trial?
FUZION is a Phase 3 randomized trial studying Tremfya, also called guselkumab, in active perianal fistulising Crohn’s disease. The week 24 data were presented at DDW 2026.
What did the FUZION trial show?
At about six months, around 27 to 28% of patients on guselkumab achieved combined fistula remission, compared with around 10% on placebo.
Does Tremfya cure Crohn’s fistulas?
No. The result is encouraging, but many patients still did not achieve complete combined fistula remission by six months. It is progress in a difficult area, not a cure for everyone.
How is guselkumab different from infliximab?
Infliximab, Remicade, blocks TNF. Guselkumab, Tremfya, blocks IL 23. They target different inflammatory pathways.
Is infliximab still important for Crohn’s fistulas?
Yes. Infliximab remains one of the most important biologics in fistulising Crohn’s disease and has landmark trial evidence.
Do Humira, Stelara and Entyvio still have roles?
Yes. Adalimumab, Humira, ustekinumab, Stelara, and vedolizumab, Entyvio, all have supportive data and are used in practice. Treatment choice depends on the patient’s disease pattern, previous response, drug levels, antibodies, safety factors and preferences.
Why does MRI matter in perianal Crohn’s?
MRI can show hidden abscesses, fluid collections and fistula branches that may not be obvious externally. This is why MRI is often central to good fistula care.
What is the main message?
Crohn’s fistulas are difficult. FUZION is important because it gives us serious modern trial data for guselkumab in a neglected and challenging area of Crohn’s disease.
1. Crohn's Disease Basics and Key Decisions
- Crohn’s Disease Treatment in Dubai
- Inflammatory Bowel Disease Overview
- Ulcerative Colitis Treatment in Dubai
2. Biologics, Advanced Treatments and Treatment Strategy
- Learn about Biologicals used in UC and Crohn’s in Dubai
- Tremfya, Guselkumab, Explained for Crohn’s and Colitis
- Rinvoq for Crohn’s and Colitis
- Stelara vs Skyrizi in Crohn’s Disease
- Vedolizumab in Crohn’s Disease Timing
- Why Not to Stay on Steroids in Crohn’s and Colitis
3. Crohn's Diet, Gut Barrier and Microbiome
- Diet and Microbiome in IBD
- Gut Microbiome in Crohn’s and Ulcerative Colitis
- Plant Based Diet and Crohn’s Disease
- Elemental Diet in Crohn’s Disease
- Can Food Help Calm Crohn’s Disease
- SIBO in Crohn’s and Ulcerative Colitis
- Leaky Gut in Crohn’s and Ulcerative Colitis
- Gut Microbiome Test
4. Related Conditions and Deficiencies
5. Diagnostic Tests and Procedures
- MRI Abdomen and MR Enterography
- CT Abdomen and CT Enterography
- Capsule Endoscopy
- Colonoscopy
- Gastroscopy
- Hydrogen and Methane Breath Test
- Diagnostic Tests for Gastrointestinal Disorders
If you wish to discuss this further or would like to make an appointment, please use the booking form on this page.